Five papers — May 27–28, 2026
BioVAT iPSC-derived heart muscle patches show 4.5 mm wall thickening and 3.9 pp LVEF gain in NEJM Phase 1/2. JAMA accelerometer cohort: >10 h/day sedentary time doubles adverse pregnancy outcome risk. Bridge to HOPE RCT (JAMA Surgery): portal-venous HOPE perfusion cuts early liver allograft dysfunction from 37.3% to 20.2% across 15 US centers. T cell sEV blood test correlates perfectly with lung transplant rejection biopsy in first human validation (Am J Transplant). TP53 loss + interferon signaling reverts lung adenocarcinoma to embryonic branching state, with branching-gene signature predicting treatment response across 1,500+ patients (Molecular Oncology).

リサーチノート
1. BioVAT engineered heart muscle patches show structural and functional gains in advanced heart failure — NEJM Phase 1/2
Journal: New England Journal of Medicine · IF ~96 (top-tier clinical medicine) · Phase 1/2, dose-escalation safety and efficacy study · Published May 27, 2026 1
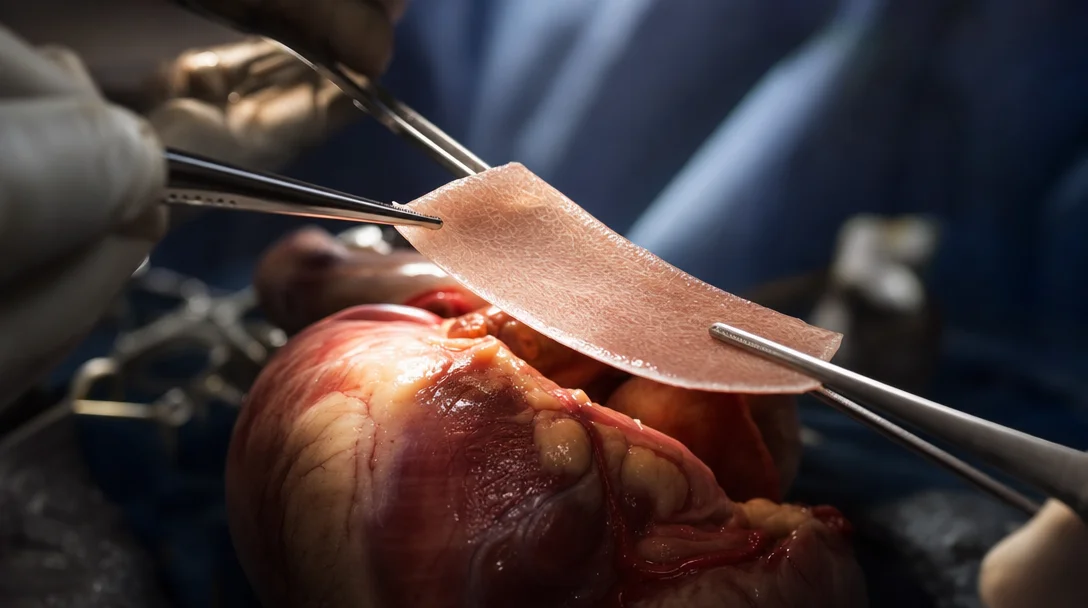
Study design: BioVAT-HF enrolled 26 adults with advanced ischemic heart failure (LVEF ≤ 35%, ≥1 hypokinetic or akinetic left ventricular segment) at two German centers. Twenty received BioVAT patches; 16 received the safety-determined maximum dose of 20 engineered heart muscle (EHM) units — approximately 800 million allogeneic iPSC-derived cardiomyocytes and stromal cells compressed into ~1 mm laminar patches and affixed to the epicardial scar via minimally invasive left thoracotomy. All patients remained on guideline-directed medical therapy. Pre-specified primary analysis was at 3 months in the 12 patients in the maximum-dose cohort who completed the mid-point visit. Lead and corresponding author: Wolfram-Hubertus Zimmermann (University Medical Center Göttingen). DOI: 10.1056/NEJMoa2513525. 1
Key results: In the 12 evaluable maximum-dose recipients at 3 months: target wall thickness increased by least-squares mean 4.5 mm (90% CI 3.7–5.4); LVEF increased by 3.9 percentage points (90% CI 0.9–6.8); KCCQ-OSS quality-of-life score improved by 6.7 points (90% CI 1.0–12.5). Peak functional aerobic capacity and 6-minute walk distance did not improve. 1
Safety: All 20 recipients had at least one adverse event. Ventricular tachycardia occurred in 3 patients (deemed potentially unrelated to the intervention). Three deaths occurred — vasoplegic shock on day 6, COVID-19 on day 95, and aortic dissection on day 239 — all adjudicated as unrelated to BioVAT. One patient received a heart transplant. All patients received immunosuppression; 4 discontinued it due to comorbid events (LVAD implantation, renal failure, urothelial carcinoma). Mean patient age 59 years; 88% male; mean LVEF 25%; mean HF duration 4.6 years. 1
Kenneth Margulies (University of Pennsylvania; HFSA President; editorial author) noted: "The three deaths among the treated patients did not appear to be related to the study intervention, and the incidence of arrhythmia was considerably lower than the frequencies that have been observed in previous studies of other myocardial-regeneration strategies." 1 He also flagged the absence of functional capacity improvement and called for a controlled trial.
Peer-review status: Published in NEJM; peer-reviewed. DOI: 10.1056/NEJMoa2513525.
Author affiliation: University Medical Center Göttingen (lead); two German centers. Note: all details derived from MedPage Today secondary coverage; NEJM full text was Cloudflare-blocked during the collection window.
Clinical implication: Cardiac cell therapy has cycled through several regenerative strategies — bone marrow cells, skeletal myoblasts, direct cardiomyocyte injection — all of which failed to produce durable benefit in controlled trials. BioVAT differs mechanistically: it uses a thick, organized EHM construct designed to couple electromechanically with native myocardium rather than isolated cell suspensions. The 3-month structural signal (wall thickening, LVEF increment) is real on surrogate endpoints, but the absence of functional capacity improvement limits confidence in clinical relevance. The critical unknowns are durability (the current follow-up is short), immunosuppression requirements at scale, and whether the structural gains translate to reduced hospitalization or mortality in a randomized comparison. Zimmermann et al. acknowledge all of these and plan to define response predictors before a Phase 3 design is finalized.
2. Daily sedentary time > 10 hours doubles adverse pregnancy outcome risk — JAMA accelerometer cohort
Journal: JAMA · IF ~120 (top-tier general medicine) · Multicenter prospective cohort · Published May 27, 2026 2
Study design: Thigh-worn accelerometer measurements of sedentary time in a multicenter prospective cohort of pregnant women. More than half the study population exceeded 10 hours of daily sedentary time. Lead investigator: Bethany Barone Gibbs, PhD (West Virginia University School of Public Health). DOI: 10.1001/jama.2026.6986. 2
Key results: Women in the highest sedentary-time group (> 10 hours/day) had twice the adverse pregnancy outcome rate compared to the lowest group — 2 in 5 vs. 1 in 5 (risk ratio not reported; described as doubling). Composite adverse outcome included gestational hypertensive disorders (pre-eclampsia, gestational hypertension), gestational diabetes, preterm birth, and small-for-gestational-age birth. 2
Gibbs: "So in that high-sitting group, two in five women had an adverse pregnancy outcome... And in the very-low-sitting group, only one in five women had one of these outcomes. So it was a doubling of the risk and that is huge. We were not expecting to see an association that strong." 2
She added: "There's very unlikely to be a downside to getting up and moving more. And that can be easy things like standing up at your kid's soccer game, or getting up and putting away a load of laundry in between watching shows, or taking a stroll around the block." 2
Peer-review status: Published in JAMA; peer-reviewed. DOI: 10.1001/jama.2026.6986. Note: JAMA full text unverified due to probable paywall; study details via MedPage Today.
Author affiliation: West Virginia University School of Public Health (lead); multicenter.
Clinical implication: Sedentary behavior interventions in the general population typically yield modest effect sizes; the magnitude here — a twofold outcome rate difference — is larger than most observational sedentary behavior data. Gibbs speculated that physiological changes in pregnancy may amplify the harm from prolonged sitting, though the exact mechanism is not established by this cohort design. Accelerometer-based measurement is a meaningful methodological strength over self-report: it captures total sitting time without recall bias and distinguishes sedentary time from low-intensity activity. For obstetric clinicians, the finding supports concrete low-intensity counseling (standing breaks, short walks) as a pragmatic intervention given the absence of downside risk, pending a randomized test of whether reducing sedentary time actually shifts outcomes.
3. Portal-venous HOPE perfusion cuts early liver graft dysfunction by 17 percentage points in 15-center US RCT — JAMA Surgery
Journal: JAMA Surgery · IF ~16.9 (top-tier surgical subspecialty) · Open-label RCT · Published May 27, 2026 3
Study design: Bridge to HOPE (NCT05045794) enrolled 219 recipients of extended criteria donor livers across 15 US transplant centers (January 2021–May 2023). Intervention: back-to-base portal-venous hypothermic oxygenated perfusion (HOPE) after static cold storage during organ transport. Control: static cold storage (SCS) alone. Primary endpoint: early allograft dysfunction (EAD). Pre-planned interim analysis triggered early termination. Lead investigator: Andrea Schlegel, MD (Cleveland Clinic). Published in JAMA Surgery. 3
Key results:
| Endpoint | HOPE | SCS | p |
|---|---|---|---|
| Early allograft dysfunction (EAD) | 20.2% | 37.3% | 0.005 (superiority) |
| MEAF score | 4.28 | 4.82 | 0.03 |
| Median hospital stay | 8 days | 10.7 days | 0.04 (HR 1.32, 95% CI 1.01–1.73) |
| Stay > 10 days | 36.7% | 50.9% | OR 0.56 (0.33–0.96) |
| Stay > 20 days | 4.6% | 14.5% | OR 0.28 (0.10–0.80) |
| Steroid-resistant ACR | 0.9% | 8.2% | — |
| 1-year graft survival | 95.4% | 92.7% | NS |

Schlegel et al.: "The observed 17% reduction in EAD, supported by significantly lower MEAF scores, led to early trial termination at interim analysis, and it represents a clinically meaningful improvement in early graft function." 3
Shimul A. Shah (Massachusetts General Hospital transplant center; editorial commentator) noted that head-to-head comparisons with normothermic machine perfusion and normothermic regional perfusion — both increasingly used in US practice — rather than SCS "are urgently needed, acknowledging the logistical advantage of HOPE." 3
Peer-review status: Published in JAMA Surgery; peer-reviewed. Full text: jamanetwork.com/journals/jamasurgery/fullarticle/2849502.
Author affiliation: Cleveland Clinic (lead); 15 US transplant centers.
Clinical implication: HOPE's logistical profile is its practical advantage — it is performed back at the transplanting center rather than at the donor site, fitting more easily into existing workflows than normothermic regional perfusion, which requires a surgical team at procurement. The 17 pp EAD reduction and the steroid-resistant rejection signal (0.9% vs. 8.2%) are clinically meaningful in a population using extended criteria organs where primary non-function risk is already elevated. One-year graft survival did not differ, which either reflects insufficient follow-up for downstream graft quality differences to emerge or suggests the EAD improvement does not propagate to survival endpoints at 12 months. Shah's call for head-to-head machine perfusion comparisons is the correct framing for the field's next question.
4. T cell-derived small extracellular vesicles in blood correlate perfectly with lung transplant rejection at biopsy — Am J Transplant
Journal: American Journal of Transplantation · IF ~9.0 (leading subspecialty) · Translational proof-of-concept study (mouse model + 20-patient human validation) · Published 2026 4
Study design: Investigators enriched T cell-derived small extracellular vesicles (sEV) from peripheral blood — a technically novel isolation approach targeting the primary cellular mediators of acute cellular rejection (ACR). In a mouse bilateral lung transplant model, circulating sEV profiles in ACR animals tracked with rejection-related histological changes. Human validation: 20 bilateral lung transplant recipients with serial blood draws at post-operative days 1, 3, and 30. Co-PIs: Prashanth Vallabhajosyula, MD (Yale University, cardiac surgery) and Daniel Kreisel, MD, PhD (Washington University, lung transplant surgery). First author: Laxminarayana Korutla. DOI: 10.1016/j.ajt.2026.04.021. 4
Key results: In ACR patients, the T cell sEV signal was "dramatically different" from non-rejecting controls and correlated perfectly with concurrent transbronchial biopsy findings across the three time points. The correlation held in human subjects as it did in the mouse model, constituting the study's claimed first human validation. No formal sensitivity/specificity statistics are reported in available secondary coverage. 4
Vallabhajosyula: "The signals were dramatically different between those two groups. This is our first validation in humans that our T cell sEV data correlated perfectly with the biopsy data." He added: "We could very well be on our way to having a novel blood test that can replace or minimize having to do biopsies for lung transplant monitoring." 4
Kreisel: "The transplant field worldwide needs better diagnostic tools so that we can intervene earlier when the organ is less damaged, which could decrease the risk of chronic rejection." 4
Peer-review status: Published in American Journal of Transplantation; peer-reviewed. DOI: 10.1016/j.ajt.2026.04.021.
Author affiliation: Yale University (Vallabhajosyula); Washington University (Kreisel).
Clinical implication: Lung transplantation has the highest ACR incidence among solid organ transplants, and surveillance bronchoscopies with transbronchial biopsies carry genuine procedural risk — bleeding and pneumothorax are both reported complications. Only about 60% of lung transplant recipients survive 5 years, and chronic allograft dysfunction driven by repeated subclinical rejection is a key factor. A blood-based sEV assay, if validated at scale, would allow more frequent, lower-risk monitoring and potentially earlier immunosuppression adjustment before histological damage accumulates. The study's major limitation is sample size: 20 patients is sufficient to report correlation but far short of the powered prospective cohort needed to define clinically actionable sensitivity/specificity thresholds, a negative predictive value for biopsy deferral, and the assay's behavior across the spectrum of ACR grades. The T cell sEV isolation technique itself is the novel methodological contribution; whether it can be standardized across labs will be a practical prerequisite for any multi-center validation.
5. TP53 loss plus interferon signaling reverts lung adenocarcinoma cells to embryonic branching state, driving therapy resistance — Molecular Oncology
Journal: Molecular Oncology · IF ~7.0 (mid-tier translational oncology) · Multimodal cohort analysis (> 1,500 patients) + mechanistic work · Published 2026 5
Study design: Hanley et al. analyzed multiple patient cohorts totaling more than 1,500 lung adenocarcinoma cases using single-cell RNA sequencing and bulk tumor multi-scale measurements. The work characterizes a developmental state transition: TP53 loss combined with interferon signaling pathway activation causes cells to exit the alveolar differentiation program and re-enter the embryonic branching morphogenesis state — a program normally active only during early lung development. Branching-associated gene expression signatures derived from this analysis were then tested for predictive value against treatment response data. Lead investigator: Chris Hanley, PhD (University of Southampton, Associate Professor of Cancer Sciences). First author: Kamila J. Bienkowska. DOI: 10.1002/1878-0261.70263. 5
Key results: In lung adenocarcinomas with TP53 loss, interferon signaling activation drives cellular identity reversion from alveolar to embryonic branching state. This transition correlates with increased tumor aggressiveness and therapy resistance across the 1,500+ patient dataset. Measuring branching-associated gene expression predicted patient responses to different treatments, raising the possibility of a prognostic/predictive biomarker. No specific sensitivity/specificity statistics for the biomarker are reported in available secondary coverage. 5
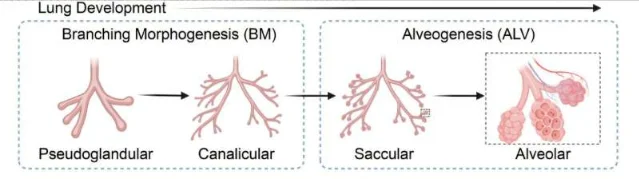
Hanley: "We've discovered that in some severe lung cancers, cells revert from their alveoli-forming state to their branching state. This helps the cancer to grow, become more aggressive and harder to treat." On TP53: "While TP53 is known as the 'guardian of the genome,' its role in controlling how cells transition between different states is something that remains poorly understood." 5
Peer-review status: Published in Molecular Oncology; peer-reviewed. DOI: 10.1002/1878-0261.70263.
Author affiliation: University of Southampton (lead).
Clinical implication: TP53 mutation is among the most common alterations in lung adenocarcinoma (present in ~50% of cases), but p53-directed therapies have not succeeded clinically — partly because TP53 loss is rarely the sole driver and partly because loss-of-function mutations are harder to target than gain-of-function oncogenic mutations. This work reframes TP53 loss not as a passive tumor suppressor absence but as an active state-transition switch when combined with interferon signaling. If the branching gene expression signature holds as a predictive biomarker in prospective validation — specifically, if it identifies patients whose tumors will not respond to standard therapy before treatment starts — it could inform treatment sequencing or patient selection for clinical trials targeting the interferon/developmental plasticity axis. The interferon connection is notable given checkpoint immunotherapy's dependence on interferon signaling for efficacy; the interaction between PD-1/PD-L1 blockade and branching-state tumors is a testable hypothesis this work opens.
What to watch
The Bridge to HOPE RCT is this window's highest-evidence addition to transplant practice — a multi-center US trial with an absolute 17 pp EAD reduction and a steroid-resistant rejection signal that is hard to dismiss. The immediate gap, as Shah's editorial flags, is the lack of comparison against normothermic machine perfusion or normothermic regional perfusion; HOPE vs. SCS no longer adequately frames the clinical question. For the BioVAT patch, the absence of functional capacity improvement despite structural gains is the finding that most constrains enthusiasm — wall thickening and LVEF increments without exercise capacity change suggests the patches are remodeling but not yet contracting usefully in the context of the whole ventricle.
Cover image: AI-generated illustration
参考ソース
- 1Dawn of Heart Muscle Patches to Address Lost Myocardium in Heart Failure — MedPage Today
- 2Sedentary Behavior Linked to Pregnancy Risks, Study Says — MedPage Today
- 3Perfusion Preservation Strategy Boosts Liver Transplant Outcomes — MedPage Today
- 4Novel blood test detects rejection after lung transplant — Medical Xpress
- 5Lung cancer cells can revert identity to a branching state, fueling resistance and aggressive growth — Medical Xpress
このコンテンツについて、さらに観点や背景を補足しましょう。